
Designing QuantumLife's first hospital-deployed AI platform
Unlocking institutional sales, multi-segment scalability, and physician-verified clinical intelligence.
0→1 Product Design
B2B/SaaS
UIUX Design
Enterprise Healthcare AI
Deployed at Gleneagles Hospital Hong Kong
Impact
Gleneagles Hospital Hong Kong — IHH Healthcare (USD $5.3B revenue, 80+ hospitals across Asia)
First institutional deployment of a physician-verified AI clinical decision support platform
From product discovery to hospital deployment in 3 months
01 Product Context
From Genomic Analysis Technology to Enterprise Clinical Platform
QuantumLife had developed AI-powered genomic analysis technology — but without a deployable product interface, the technology remained uncommercial. Securing the company's first institutional customer required translating multi-omics AI into a platform that hospital procurement could approve, physicians would adopt within existing consultation workflows, and the business could scale without on-site support.

This translation posed three simultaneous constraints:
The platform had to satisfy institutional compliance requirements
Constraint 1
Integrate into existing clinical workflows rather than impose new ones
Constraint 2
Remain viable for a startup with limited engineering resources
Constraint 3
02 Leading Product Strategy and Interface Design
I led product strategy and end-to-end interface design as the designer on the project. For Longevity.Omics, I independently drove:
✍️Product Strategy
🔍UX research
🧩IA (Information Architecture) Design
🏥Clinical Interface Design
👤Enterprise Admin System Design
📇Design System
🛠️Developer Handoff and QA
I worked directly with QuantumLife's CEO and engineering team, translating business requirements and physician research into a deployable platform within three months.
03 Stakeholder Constraints
Three Conflicting Requirements, One Platform Architecture
Enterprise healthcare AI products must reconcile genuinely conflicting stakeholder requirements. Identifying these structural tensions — not just interface preferences — defined the initial design challenge.

The design challenge was not selecting one stakeholder to optimize for — it was identifying an architecture that could
satisfy all three within a single platform.
QuantumLife's resource constraints made this non-negotiable:
separate products for different hospital sizes were not viable.
03 Architectural Pivot
How Physician Feedback Invalidated the Unified Portal Assumption
The initial approach followed standard platform logic: a unified physician portal consolidating patient management, test ordering, report review, and billing into a single interface.


We prototyped it. We brought it to physicians at partner hospitals for validation testing. Across multiple sessions, one piece of feedback emerged consistently:


The surface-level response would have been to remove the payment module from the physician portal.
However, this feedback exposed a deeper structural question: if physicians don't handle payments, a separate operational layer must exist within the hospital. The unified portal wasn't missing a feature — it was built on an incorrect model of hospital operations.
04 Institutional Research
Mapping Administrative-Clinical Separation Across
A consistent structural pattern emerged across every institution studied. Large hospitals maintain dedicated departments for finance, billing, and procurement — entirely separate from clinical operations. Physicians operate exclusively within the clinical domain.
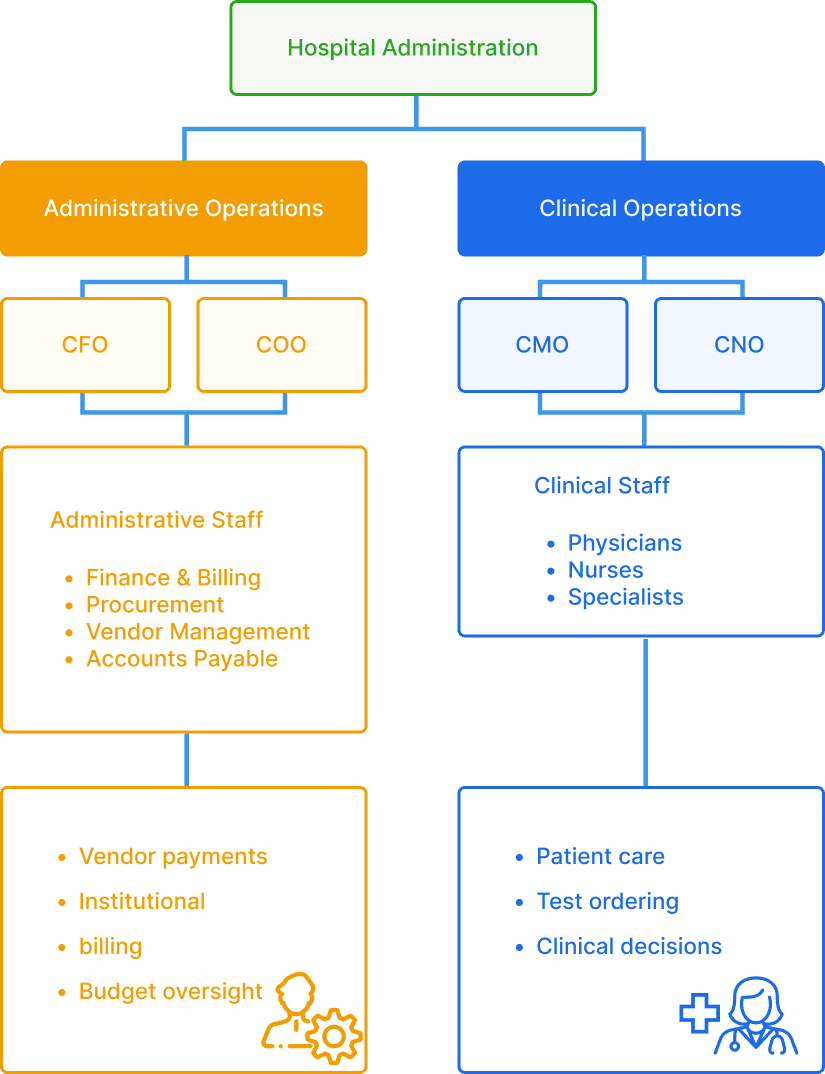
In large hospitals, entire departments handle finance, billing, procurement, and vendor management.

Even in clinics with one or two administrative staff, the person handling billing is not the physician. The scale compresses, but the boundary stays.
Critical Discovery
Despite different scales and role complexity, the separation between administrative operations and clinical work is universal — and it's not organizational preference.
This finding redefined the architectural requirements. The platform needed two distinct interfaces — administrative and clinical — operating within a shared infrastructure, mirroring the organizational separation that exists in every healthcare institution regardless of scale.
05 Platform Architecture
One Architecture, Two Portals, Every Hospital Size
The institutional research directly informed the architectural restructure. Rather than a unified interface with configurable permissions, the platform separated administrative functions from clinical workflows at the foundational level — mirroring the operational separation inherent in hospital organizations.
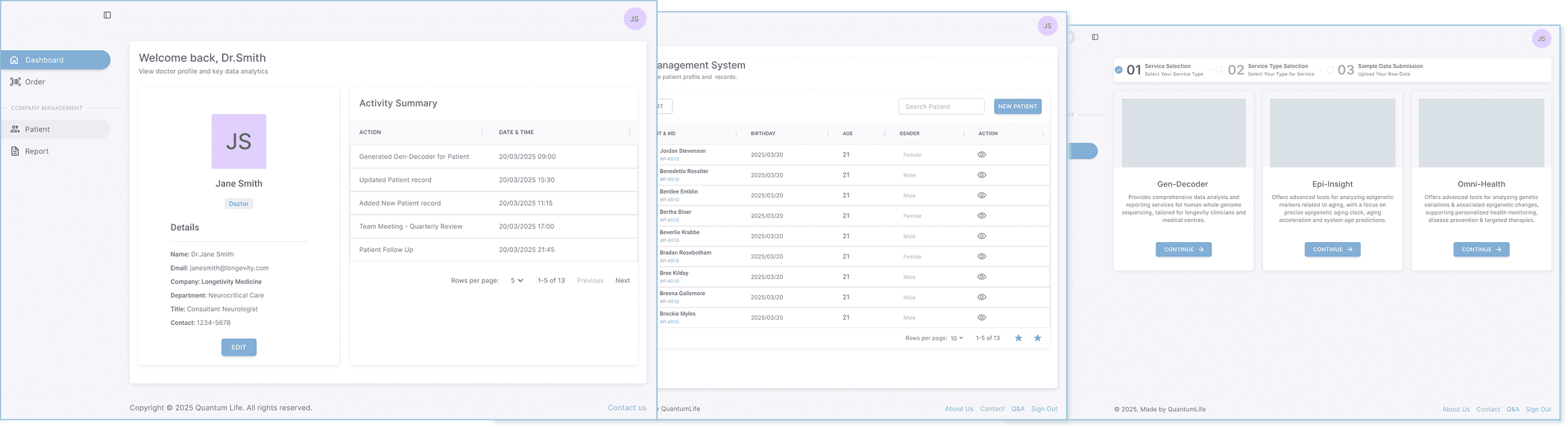
Doctor Portal
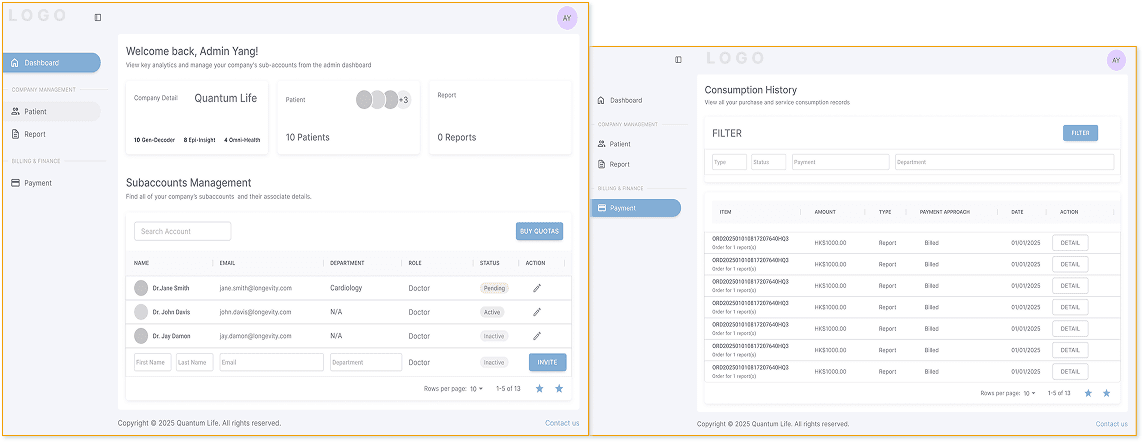
Amin Portal
This solved the three-way constraint:

For Physicians
A clinical workspace isolated from administrative functions, physicians interact exclusively with patient data, AI analysis, and clinical decision tools.
For hospital administrators
Centralized oversight and compliance controls through the Admin Portal — institutional requirements satisfied without introducing administrative functions into the clinical interface.
For QuantumLife
One platform architecture that serves both large hospitals and boutique clinics. The admin layer scales up or down based on institutional size. The clinical layer stays the same regardless.
Trade-off
Building two portals instead of one increased initial development scope — the admin portal (dashboard, sub-account management, payment tracking) represented additional engineering investment that a single-portal architecture wouldn't require.
Outcome
A single platform architecture now serves every hospital size.
Large hospitals receive institutional compliance through the admin portal. Boutique clinics operate with a simplified administrative layer. The clinical interface remains identical across deployments. This eliminated the need for segment-specific products — avoiding what would have been a resource-prohibitive development path for an early-stage company.
The architecture also supports feature-level modularity. Gleneagles manages ordering through their internal hospital system, so the Gleneagles deployment removes the Order function from the doctor portal entirely. Smaller clinics without internal ordering systems retain it. The platform adapts to each institution's existing operational infrastructure rather than imposing a fixed feature set.
06 Clinical Interface Design
Designing for the Physician-Verified Consultation Workflow
The clinical interface represents the critical adoption point in QuantumLife's B2B2C model. Physician adoption during consultations determines whether hospitals perceive ongoing clinical value — and consequently, whether institutional contracts renew.
No existing product category addressed this moment. Sequencing labs deliver data without clinical interpretation. Direct-to-consumer platforms generate automated reports that bypass physician judgment. Manual consultation preserves clinical authority but cannot process millions of genetic variants. QuantumLife's physician-verified model positions AI analysis and physician clinical judgment within the same workflow — a product category that did not previously exist.
Every interface decision in this section operates under three simultaneous constraints:
Compatibility with existing clinical consultation workflows
Constraint 1
Preservation of physician authority over AI-generated content
Constraint 2
Completion within a standard 15-20 minute consultation window
Constraint 3
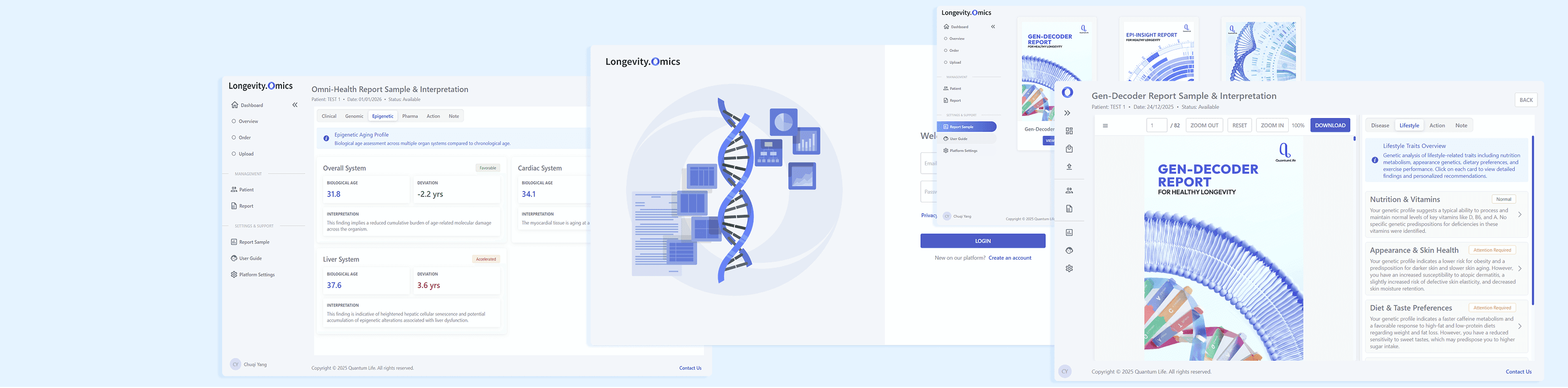
06.1 Gen-Decoder — Dual-Panel Validation Workspace
Sequencing labs produce reports containing tens of thousands of genetic variants in highly technical terminology — uninterpretable by patients and impractical for most physicians without specialized genetics training.

A single person carries 4-5 million variants, and multiple variants often point to the same clinical outcome. Tracking these cross-references across a full dataset exceeds reliable human capacity, even for specialists.
This is the problem QuantumLife's AI solves. It performs the cross-analysis that human cognition cannot do reliably — synthesizing variants across multiple omics datasets to surface clinically meaningful patterns.
But AI analysis alone isn't a product. Patients need a physician to contextualize what the findings mean for their specific situation, decide what requires intervention, and explain it in terms they can act on. QuantumLife's model is physician-verified: AI handles the analysis that exceeds human cognitive capacity, physicians provide clinical judgment and patient communication.
The interface for Gen-Decoder Report sits at this intersection. It needs to do four things simultaneously:
Accuracy
The actual patient report, not only a preview
Efficiency
Complete verification within a 15-20 min consultation
Trust
Traceable reasoning behind every recommendation
The interface uses a dual-panel workspace. Left panel: the patient's actual report — the document they will receive. Right panel: AI analysis organized for physician review. The physician reads the AI's interpretation on the right while seeing exactly what the patient sees on the left.
Accuracy
The left panel displays the actual patient-facing report. Physicians verify output quality during the consultation workflow, not retrospectively. In a model where physicians stake professional credibility on AI-generated content, real-time verification is a prerequisite for clinical adoption — not a feature enhancement.

Efficiency
The right panel distills complex genetic findings into scannable clinical summaries. Each condition surfaces a brief clinical description, risk factors, and disease classification — eliminating raw variant codes from the physician workflow. Physicians assess the clinical picture without interpreting sequencing notation, completing review within consultation time constraints. The interface needed to outperform the alternative workflow, not merely improve upon it.


Color coding distinguishes risk factors, prevention strategies, and attention items at a glance. Variant locations and their clinical consequences are labeled concisely for quick scanning.
Trust - AI credibility
Physicians can create editable action plans based on the patient's current situation. A patient with a genetic skin condition who currently has a broken leg needs different immediate guidance than the AI's default recommendation. The action plan button gives physicians space for clinical judgment that goes beyond — or overrides — AI suggestions.

Trust - Clinical credibility
Physicians can create editable action plans contextualized to the patient's current clinical situation. A patient with a genetic skin condition who currently has a broken leg requires different immediate guidance than the AI's default recommendation. The action plan interface provides the mechanism for clinical judgment that extends beyond — or overrides — AI-generated suggestions. Editable action plans constitute the concrete differentiation between a physician-verified platform and an automated report generator — this distinction represents QuantumLife's competitive moat in the clinical decision support market.

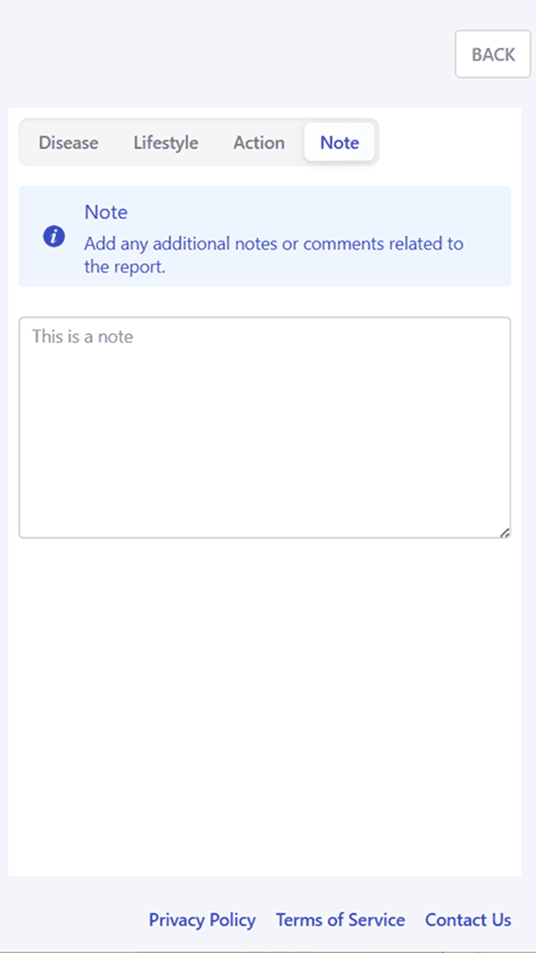
The Action tab provides an editable default recommendation plan — physicians modify based on patient context, with a dedicated Note area for clinical annotations.
06.2 Omni-Health — Multi-Dimensional Clinical Decision
Gen-Decoder and Epi-Insight provide diagnostic analysis — identifying genetic risks and biological aging status. Longevity medicine, however, requires prescriptive guidance: which risks demand immediate intervention, what specific actions optimize an individual's healthspan, and how should interventions be prioritized and monitored.
Omni-Health synthesizes all patient data — lab results, Gen-Decoder findings, Epi-Insight aging assessments — into a comprehensive clinical action strategy. Its design innovation operates at the information architecture level rather than the interface level. The strategic challenge was organizing multi-dimensional data into a coherent clinical decision workflow.
Four architectural principles:
Layered Information Flow:
Separate diagnostic inputs from prescriptive outputs. Clinical and Genomic tabs position first, establishing patient baseline through uploaded laboratory results and static genetic risks before AI-driven analysis.
Intelligent Filtering:
Interface selectively surfaces clinically actionable findings, filtering comprehensive datasets to clinical priorities.
Contextual Integration:
Each tab provides a focused view while maintaining connection to the complete patient picture.
Flexible Navigation:
Tab sequence establishes logical first-consultation workflow. However, interface supports non-sequential access for follow-up consultations.
Tab sequence and specific design decisions:



Implement Layered Information Flow — physicians establish patient baseline (current clinical status, inherited genetic risks) before moving to AI-driven analysis and intervention planning.
Clinical & Genomic tabs:
Color hierarchy guides attention: Red (accelerated aging) > Green (favorable) > Gray (normal). System displays only three categories: Overall System, Favorable organ, Accelerated organ. Physicians scan priority systems instead of reviewing every organ.
Epigenetic tab:


Two-tier prioritization. High-priority items (immediate dose adjustments) visually separated from moderate-priority items (consider during relevant prescribing). Prevents alert fatigue while ensuring nothing safety-critical is missed.
Pharma tab:


Positioned last deliberately. AI-generated 6-Pillar intervention plan synthesizes insights from all preceding tabs. Placing it after comprehensive assessment ensures recommendations are contextualized, not premature. All fields are editable — physicians modify based on patient context, compliance likelihood, and resource availability.
Action tab:
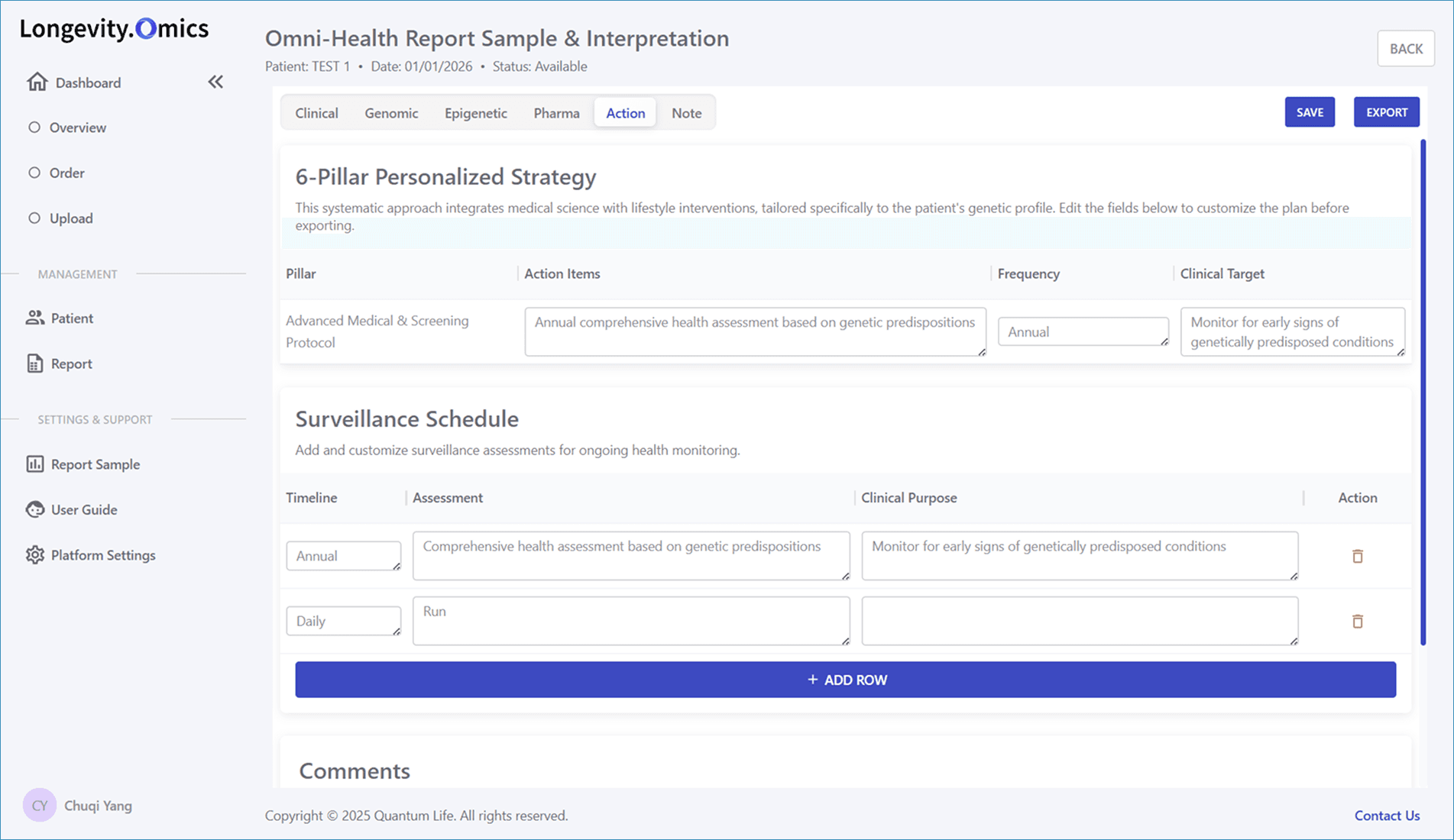
The tab sequence follows the physician's existing clinical reasoning order — current health status, then inherited risks, then aging markers, then medication implications, then comprehensive action plan. This mirrors how physicians already structure longevity consultations, supporting their existing cognitive workflow rather than imposing a new sequence.
Direct access to any tab . This supports both comprehensive initial assessments and focused follow-up monitoring, where physicians access only the relevant dimensions without repeating completed reviews.

Flexible Navigation:
Competing clinical decision support tools provide siloed analysis — separate genomic risk reports, aging assessments, and drug interaction databases that physicians must consult independently. Omni-Health synthesizes all dimensions into a unified clinical decision workflow, transforming discrete diagnostic outputs into an integrated intervention strategy.
This integration converts one-time diagnostic reports into an ongoing clinical decision support relationship — the structural basis for recurring institutional revenue.
07: Supporting Infrastructure
Standard Enterprise Patterns for Operational Independence
Beyond the core clinical interface, the complete operational infrastructure required design: patient management, service ordering, and report management for the Doctor Portal; dashboard, sub-account management, and payment tracking for the Admin Portal.
These interfaces employ standard enterprise patterns — data tables, search filters, status indicators — intentionally. Design restraint reserves cognitive novelty for the clinical decision support interface, where data complexity genuinely demands new solutions. Standard patterns also minimize training overhead — critical for a platform designed to operate without dedicated QuantumLife support staff at each deployment site.





BUSINESS IMPACT
08: Deployment Outcomes
First Institutional Validation of the B2B2C Platform

Gleneagles Hospital Hong Kong IHH Healthcare — USD $5.3B revenue, 80+ hospitals across Asia
The Longevity.Omics platform enabled QuantumLife to secure its first institutional customer, validating both the B2B2C commercial model and the dual-tier architectural approach.
What the deployment validated:
The complete commercial path — from sequencing lab to AI analysis to physician consultation to patient delivery — functions as designed.
B2B2C Model
Institutional willingness to purchase physician-verified AI platforms confirmed.
Platform completion within existing consultation workflows confirmed.
Physician Adoption
Clinical decision support interface achieved physician validation at a major hospital system.
Operational Independence
Admin portal enables institutional self-management — a prerequisite for scalable unit economics across deployments.
Platform operates without dedicated QuantumLife support staff on-site.
Institutional Architecture
The same architecture serves boutique clinics without structural modification.
Dual-tier architecture satisfied Gleneagles' enterprise compliance requirements while preserving clinical interface simplicity.
Physician-verified AI clinical decision support — where AI analysis and physician clinical judgment coexist within the same workflow — validated as a viable product category in institutional healthcare.
New Product Category